
Copy of Nephrology Module 2
Quiz Summary
0 of 32 Questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 32 Questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
| Average score |
|
| Your score |
|
Categories
- Not categorized 0%
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
- 22
- 23
- 24
- 25
- 26
- 27
- 28
- 29
- 30
- 31
- 32
- Current
- Review
- Answered
- Correct
- Incorrect
-
Question 1 of 32
1. Question
A 16-year-old girl is referred to clinic complaining of generalised muscle weakness, fatigue and polyuria. Her blood pressure in clinic is measured at 90/74 mmHg. Investigations:
- Serum sodium 127 mmol/l
- Serum potassium 3.0 mmol/l
- Serum urea 7.2 mmol/l
- Serum creatinine 110 umol/l
- Serum chloride 92 mmol/l ( 97-108 mmol/l)
- Serum bicarbonate 34 mmol/l ( 22-28 mmol/l)
- Urine sodium 160 mmol/l ( 40-130 mmol/l)
- Urine calcium 12.0 mmol/24hr (2.5-8.0 mmol/24hr)
Which of the following is the most likely diagnosis?
CorrectIncorrect -
Question 2 of 32
2. Question
A patient in the Emergency Department has the laboratory results shown below:
- Serum Sodium 130 mmol/L [136 – 146 mmol/L]
- Serum Potassium 6.5 mmol/L [3.5 – 5.0 mmol/L]
- Serum HCO3 14 mmol/L [22 – 28 mmol/L]
- Serum Chloride 115 mmol/L [95 – 107 mmol/L]
- Venous pH 7.19 [7.34 – 7.44]
- PCO2 42 mmHg [35 – 45 mmHg]
- Base excess 10 mmol/L [-3- + 3 mmol/L]
Which of the following is the most likely cause of the acidosis?
CorrectIncorrect -
Question 3 of 32
3. Question
A 16-year-old man presents with facial oedema and dark urine two weeks after a bout of tonsillitis. He has been anuric for 18 hours. Initial investigations confirm acute renal failure with markedly elevated serum urea and creatinine. His serum potassium is elevated at 6.8 mmol/L.
Which of the following intervention is most likely effective in reducing total body potassium?
CorrectIncorrect -
Question 4 of 32
4. Question
As glomerular filtration rate (GFR) declines, urinary creatinine clearance overestimates GFR because creatinine is:
CorrectIncorrect -
Question 5 of 32
5. Question
A 30 year old male patient is oliguric three days post cadaveric renal transplant.His creatinine has not improved since the operation. He undergoes a MAG3 renal scan which reveals excellent uptake and therefore perfusion but no excretion.
What is the most likely cause for this failure to improve?
CorrectIncorrect -
Question 6 of 32
6. Question
Which one of the following drugs may be cleared by hemodialysis?
CorrectIncorrect -
Question 7 of 32
7. Question
Acute renal failure as a result of gentamicin use most frequently results from which of the following mechanism?
CorrectIncorrect -
Question 8 of 32
8. Question
A 50-year-old man presenting for an insurance medical examination is found to be hypertensive with a resting blood pressure of 170/110 mmHg. He takes no medication.
The following laboratory investigations were obtained while on a normal diet:
- serum potassium 2.8 mmol/L [3.5-5.0]
- serum sodium 145 mmol/L [135-145]
- serum creatinine 0.095 mmol/L [0.080-0.120]
- urinary potassium 65 mmol/L
- urinary sodium 80 mmol/L
- plasma renin 5 mU/L [8-70]
- plasma aldosterone 1000 pmol/L [ambulant 350-700]
Which one of the following diagnoses best fits the clinical picture?
CorrectIncorrect -
Question 9 of 32
9. Question
A 35-year-old man is found to be hypertensive with a blood pressure of 180/110 mmHg. At presentation, on no treatment, the following results are obtained:
- serum potassium 3.3 mmol/L [3.5-5.0]
- urinary potassium 40 mmol/24 h [<30]
- plasma aldosterone 620 pmol/L [supine 50-450]
- plasma renin 4 mU/L [ambulatory 5-75]
The most appropriate investigation is to measure:
CorrectIncorrect -
Question 10 of 32
10. Question
A 43-year-old woman presents with a six month history of hypertension which has been difficult to control. She is now taking three agents for her blood pressure control. She has a serum potassium of 2.7 mmol/L [3.6 – 5.2 mmol/L] and you are concerned about primary hyperaldosteronism(Conn’s syndrome).
Which of the following medications is most likely to interfere with the interpretation of an aldosterone:renin ratio result?
CorrectIncorrect -
Question 11 of 32
11. Question
A patient with primary aldosteronism secondary to a unilateral adrenal hyperplasia undergoes an adrenalectomy.
Which biochemistry marker is most likely to improve post-surgery?
CorrectIncorrect -
Question 12 of 32
12. Question
Which of the following is the main site of sodium reabsorption in the nephron?
CorrectIncorrect -
Question 13 of 32
13. Question
A man comes to your clinic to get some dietary advise about what he should or should not eat after a recent admission with calcium oxalate stones in his kidney.
The following advise would be appropriate, except?
CorrectIncorrect -
Question 14 of 32
14. Question
Which of the following structure is the primary site of action for acetazolamide?
CorrectIncorrect -
Question 15 of 32
15. Question
In 2004, the ADQI formulated the RIFLE criteria to allow for acute kidney injury (AKI) to be objectively and uniformly defined. The implication of this classification is that a progression down the RIFLE criteria is associated with the following except?
CorrectIncorrect -
Question 16 of 32
16. Question
The concomitant use of which medication will increase the risk of lithium toxicity in the blood?
CorrectIncorrect -
Question 17 of 32
17. Question
Frusemide blocks which of the following co-transporter?
CorrectIncorrect -
Question 18 of 32
18. Question
Which of the following is the correct order of events in the reninangiotensin system in response to low blood pressure?
A) Kidneys reabsorb sodium and water uptake is increased
B) The kidneys sense low blood pressure.
C) Renin is released into the blood and produces Angiotensin I.
D) Release of Aldosterone, ADH, and thirst stimulation.
E) Angiotensin Converting Enzyme (ACE) converts Angiotensin I to Angiotensin II.
CorrectIncorrect -
Question 19 of 32
19. Question
A 19 year old girl presents with weakness.She is on no medications and has 4 siblings.One sister has had low potassium levels.Physical exam and BP are normal.
Investigations:
- Sodium 141
- Potassium 2.4
- Cl 98
- Bicarbonate 32
- Calcium 2.3
- Mg 0.35
Urine: Na 60, K 50, Cl 100
Prostaglandin E normal
What is the most likely diagnosis?
CorrectIncorrect -
Question 20 of 32
20. Question
A 56 year old woman is on hemodialysis for end stage renal failure due to diabetes.
Investigation reveals:
- Hb of 90g/L
- Ferritin of 80(15-180 g/L)
- Transferrin saturation 20%(15-46%)
What is the most appropriate treatment?
CorrectIncorrect -
Question 21 of 32
21. Question
Erythropoietin is predominantly made from which type of cell in the kidney?
CorrectIncorrect -
Question 22 of 32
22. Question
A 65-year-old woman, established on haemodialysis for nine months, is maintained on erythropoietin 4,000 units twice a week intravenously. Previously her haemoglobin (Hb) had remained steady in the range of 105 – 115 gm/L.
She now presents with a Hb of 89 gm/L on routine testing. There have have been no changes to her erythropoietin dose or other medications.
Her iron profile are as follow:
- mean corpuscular volume (MCV) is 84 fL [78- 98]
- serum iron is 13 micromol/l [13-35],
- iron saturation is 18% [15- 46],
- serum ferritin is 630 microg/l [20-300] and
- reticulocyte count is 30 x 109/L [12-100].
Which of the following is the most likely explanation for her erythropoietin resistance?
CorrectIncorrect -
Question 23 of 32
23. Question
A 16-year-old post pubertal boy has chronic renal failure with a serum creatinine of 300 micromol/L due to glomerulonephritis. Two years ago his creatinine was 100 micromol/L and one year ago it was 200 micromol/L.
He wants to complete his schooling in two years time before undergoing pre-emptive living related transplantation. He is growing on the 25th percentile for height and the 10th for weight (having gained height but not weight in the last year). His blood pressure is 140/105 mmHg and he has 2.0 g per day of proteinuria. His dietary protein content is 2 g/kg/day.
His serum chemistry are as follow:
- sodium 140 mmol/L [135-150]
- potassium 4.0 mmol/L [3.5-5.0]
- chloride 105 mmol/L [90-110]
- urea 45 mmol/L [<6]
- creatinine 0.3 mmol/L [0.05-0.12]
- haemoglobin 90 g/L [120-150]
- calcium 2.4 mmol/L [2.26-2.56]
- phosphate 2.6 mmol/L [0.94-1.37]
- parathyroid hormone 70 pg/ml [2-7]
Which one of the following will have no effect on the progression to end-stage renal failure?
CorrectIncorrect -
Question 24 of 32
24. Question
What is the predominant cause of anaemia in chronic renal failure?
CorrectIncorrect -
Question 25 of 32
25. Question
A 23-year-old woman presents with generalised swelling. Over the last three days she has felt tired, has experienced bilateral loin pain and has noticed darkening of her urine. She has had a skin infection on her knee which has been slow to resolve.
On examination, she has mild generalised oedema, a blood pressure of 170/115 mmHg and tenderness in the loins. The skin lesion is still encrusted and erythematous. Urinalysis shows ++proteinuria and ++blood. Other examination is unremarkable.
Investigations show:
Full blood count normalSerum biochemistry:
- sodium 135 mmol/L [137-146]
- potassium 5.1 mmol/L [3.5-5.0]
- chloride 102 mmol/L [98-108]
- bicarbonate 21 mmol/L [26-30]
- urea 44.0 mmol/L [3.5-8.5]
- creatinine 0.72 mmol/L [0.06-0.12]
- albumin 35 g/L [35-45]
- total protein 60 g/L [55-90]
Microurine shows:
- red blood cells >100 per high power field [0-1]
- white blood cells 10-50 per high power field [0-1]
- red cell casts present [0]
Serological investigations show:
- antinuclear antibody (ANA) antineutrophil cytoplasmic antibody (ANCA) negative
- antistreptolysin-O titre (ASOT) not elevated
- antiDNAse-B titre 200 U [<30]
- cryoglobulins positive
- complement component 3 (C3) 0.30 g/L [0.55-1.20]
- complement component 4 (C4) 0.18 g/L [0.20-0.50]
- throat culture negative
Apart from control of blood pressure, fluid and electrolyte management and acute dialysis if indicated, the most appropriate therapy for this renal disease is:
CorrectIncorrect -
Question 26 of 32
26. Question
A 15-year-old teenager is admitted to hospital because he has been lethargic for the past three to four weeks. He appears to be thirsty all the time with recent weight loss. He has been getting up to pass urine three times each night for the past two weeks. There is no history of drug ingestion or infection. There is no past history of note. Clinical examination is unremarkable.
His initial investigations show the following:
Serum:
- sodium 135 mmol/L [135-146]
- potassium 3.0 mmol/L [3.5-5.0]
- urea 16.0 mmol/L [3.2-7.7]
- creatinine 60 umol/L [45-90]
- glucose 23.5 mmol/L [2.5-7.0]
urinalysis 1+ protein, no blood, moderate glucose
urine microscopy 40 white cells,The most likely diagnosis in this patient is:
CorrectIncorrect -
Question 27 of 32
27. Question
A young woman presents with thirst and polyuria. Following overnight water deprivation, which one of the following is the best indicator that she has partial (and central) diabetes insipidus (Arginine Vasopressin Deficiency) rather than psychogenic polydipsia?
CorrectIncorrect -
Question 28 of 32
28. Question
A young man is identified as having haematuria (>50,000 red blood cells/mL). This is associated with a trace of protein on urine dipstick testing on several occasions. His blood pressure is 110/70 mmHg and no abnormalities are detected on physical examination.
His serum biochemistry results are as follow:
- creatinine 0.08 mmol/L [0.08-0.12]
- urea 4.5 mmol/L [4.0-8.0]
- sodium 135 mmol/L [135-145]
- potassium 3.5 mmol/L [3.5-5.0]
- chloride 95 mmol/L [93-105]
- glucose 3.5 mmol/L [3.5-7.0]
What is the most likely diagnosis?
CorrectIncorrect -
Question 29 of 32
29. Question
Persistent reduction of serum complement component 3 (C3) is most strongly associated with which one of the following forms of glomerulonephritis?
CorrectIncorrect -
Question 30 of 32
30. Question
A 56-year-old woman presents with generalised swelling including legs, hands and face and no other relevant history. She has had a normal examination two years prior. Apart from oedema, the only abnormality on current examination is a blood pressure of 170/105 mmHg.
Urinalysis shows protein ++++, blood ++, dysmorphic red cells, red cell casts and granular casts.
Her blood tests are as follow:
- urea 18 mmol/L [3.0-8.5]
- creatinine 0.205 mmol/L [0.040-0.100]
- total protein 55 g/L [63-80]
- albumin 25 g/L [35-45]
- cholesterol 7.5 [<5.5]
- triglycerides 2.5 [0.10-2.10]
- ANA, ANCA (anti-neutrophil cytoplasmic antibody) and anti glomerular basement membrane assays are all negative.
What is the most likely renal pathology?
CorrectIncorrect -
Question 31 of 32
31. Question
A 16-year-old girl presents to the emergency department with swollen eyes and ankles for one week. She has been lethargic and complained of back and right flank pain for approximately 10 days. Examination reveals a well grown adolescent with blood pressure 120/84 mmHg. She has pitting oedema up to her thighs and her liver is palpable 2 cm below the right costal margin and is tender. Urine microscopy shows 400 red cells, red and white cell casts and 4+ protein.
Blood tests show:
- haemoglobin 85 g/L [115-150]
- white cell count 4.62 x 109/L [4.40-12.50]
- segmented neutrophils 3.33 x 109/L [1.50-7.40]
- lymphocytes 1.02 x 109/L [1.50-4.70]
- platelet count 110 x 109/L [150-400]
- plasma creatinine 0.10 mmol/L [0.04-0.08]
Which one of the following is the most likely diagnosis?
CorrectIncorrect -
Question 32 of 32
32. Question
A 45-year-old woman has had six episodes of nephrotic syndrome over the last five years. The initial episodes responded promptly and completely to oral prednisone, but recent episodes have responded more slowly. At the completion of her last course of prednisone two weeks ago, urine protein was 500 mg/day.
The trichrome-stained renal biopsy is shown below.
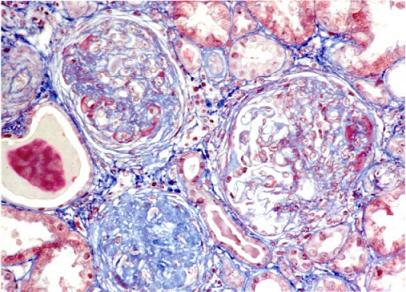
What is the most likely diagnosis?
CorrectIncorrect